

Physiotherapy for Geriatrics


SLMC and APC (LimitedReg) Physiotherapist (BSc. Hons in Physiotherapy)
Charmi Kodithuwakkuarachchi an experienced Physiotherapist with 10+ years in the fields of Orthopaedic, Rheumatology and rehabilitation, Medical and Surgical ICU management, Neuro and Musculoskeletal conditions, Out-patient departments and Paediatric care settings in four major hospitals in Sri Lanka. And also she is driven and determined to provide optimum care for her clients with hands-on skills in joint mobilization, soft tissue massage, therapeutic exercises prescription and patient education.
Her Physiotherapy role includes giving individualized tailored treatments for the specific need providing a holistic approach in patient care.
Completion of physio assessment pre and post intervention. Mobility reviews and post hospital reviews.
Prescribing equipment to improve function and quality of life.
What is Aging?
A feature of an organism’s design that has evolved over time and is beneficial to the survival of species.
Or
A disease or defect that confers no survival benefit.
In 1991, the book Evolutionary Biology of Aging offered the following definition of aging: a persistent decline in the age-specific fitness components of an organism due to internal physiological deterioration (Rose, 1991)
Myths and stereotypes about aging/old age
- Starts at 65 years
- Is a disease
- Always brings mental impairments
- Enjoying the life is a sin at old age
- Have poor attitudes
- Old people are powerless
- Nothing can be done to modify aging
- Government always has a youth-focused attitude
Stages of Life Span
- Adolescence – The 6 years following puberty
- Adulthood – Between 20 to 65 years
- Senescence – From 65 years to death
65 – 74 young old
75 – 84 old old
85 – Oldest old
As Physiotherapists,
- Although the process is unavoidable, by better understanding the process, we are able to positively influence aspects that maintain or engender better health and wellness as a person ages, treating and improving symptoms of common conditions associated with ageing.
Age related geriatric conditions
Musculoskeletal Disorders
Osteoporosis
Osteoarthritis
Rheumatoid Arthritis
Gout Arthritis
Respiratory Disorders
COPD
Asthma
Pulmonary embolism
Cardiovascular Disorders
Acute MI
Coronary heart disease
Hypertension
Cognitive cardiac failure
Neurological Disorders
Stroke
Parkinson’s Disease
Peripheral Neuropathy
Cognitive Deficits
Dementia
Alzheimer’s disease
Other complications
Falls in elderly
Diabetes in elderly
Incontinence
Physical therapy focuses on functional mobility while maintaining safety, enabling the older adult to enjoy a longer life by living it more independently and with less pain.
Possible indications for geriatric physical therapy referral. Please go see a Physiotherapist if you have following –
Recent fall or history of falls
- Deficits in strength or range of motion
- Loss of mobility or ambulation requiring an assistive device
- Musculoskeletal pain
- Difficulty with transfers
- Orthotic or prosthetic needs
- Open wound
- Neurologic disorder
- Dizziness or balance deficits
- Decreased endurance for Activities of Daily Living. (ADLs)
- Bedbound status
- Need for adaptive equipment to enhance safety and function
- Incontinence
- Frailty
Aims of Physiotherapy
Reduce pain
- Improve sensation, joint proprioception
- Increase overall fitness through exercise programs
- Suggest assistive devices to promote independence
- Recommend adaptations to make the person’s home accessible and safe
- Prevent further decline in functional abilities through education, energy conservation techniques, joint protection
- Increase, restore or maintain range of motion, physical strength, flexibility, coordination, balance and endurance
- Teach positioning, transfers, and walking skills to promote maximum function and independence within the person’s capability
Therapeutic intervention
- Range of motion exercises
- Stretching exercises
- Mobilizing exercises
- Strengthening exercises
- Aerobic exercises
- Energy conservation techniques
- Posture correction
- Gait training and assistive devices
- Prosthetics and Orthotics
- Recommendations for cognitively active life style
- Electrotherapeutic modalities
Always select a Aerobic Exercise programme as an Elderly person –
1st Step – Aerobic warm up 10 min
Slow walking followed by Total body stretching
2nd Step – Aerobic Exercises
30 minutes of Strengthening and Range of Motion Exercises (Considering individual needs and abilities)
Weight-bearing Low-impact exercises ex- stationary stepping or
Non-weight bearing Non-impact exercises ex-seated on a chair
3rd Step – Cool down 10 min
Slow walking with slow breathing relaxation exercises
Common Exercises that can be done by a Healthy Elderly Person
Please note these exercises could defer according to individual’s physical, psychological fitness levels.
- Continuing a chosen set of exercises at least 3 to 4 days a week (we do not recommend all 7 days for your workouts as you need more time to recover) will prevent you from risk of falls, improve your balance and will also make you comfortable with your activities of daily living.
- Avoid High impact Weight bearing Anaerobic exercises as much as possible. Ex – Jumping, Fast jogging or Running exercises.
- This is a very simple illustration of few common active exercises where mostly patient can perform by him or herself. There could be indications and contra-indications. Please meet your Physiotherapist for an individualized, adjusted exercise prescription after a thorough physical assessment.
- Warm up(with whole body stretch) and Cool down(with whole body stretch and relaxing) for 10minutes each is a MUST before and after the exercise programme.
Muscle Strengthening Exercises
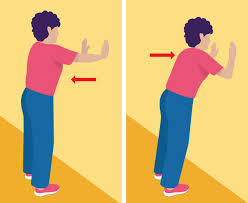
1) For Upper Limbs – Active Exercises (3 to 4 days per week)
- Wall Push-ups à10 repetitions, 2 times a day.
- Theraband exercises (be seated on a chair)à Stretch the theraband for 10 to 15 seconds, slowly release, 10 repetitions twice a day.
- Free Weights (Dumbbells) à Elbow flexion and Extension, 1kg or 2kg maximum, 10 repetitions, 2 times a day.


2) For Lower Limbs – Active Exercises (3 to 4 days per week)
- Isometric Quadricep exercises (seated or lying down on ground)
Press down a rolled towel or a sand bag kept under knee, hold for 10 to 15 seconds, slowly release to starting position, repeat for 10 times twice a day for both knees.


Hip abductor muscle strengthening


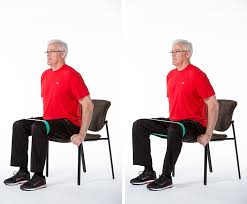
- Be seated on a chair, use a theraband wrapped around both legs (just above knee joint as shown in the pic) à widen your hips against the resistance of the theraband, hold for 10 seconds, slowly release, repeat 10 times, twice a day.
- Stand up holding on to a fixed chair with both hands Or Lying down side ways à Lift 1 leg away from your body sideways, hold for 10 seconds, back to starting position, repeat for 10 times for both lower limbs. Twice a day.
- Hip Flexor muscle strengthening
- Leg raises (Hip 90 Knee 90) seated on a chair or holding on to a fixed chair from both hands à hold up to10 seconds, leg back on ground, repeat 10 times for both legs, twice a day.


- Heel(Calf) raises (seated on a chair or holding on to a fixed chair from both hands) à stand on tiptoes, maintain position for 10 seconds, repeat for 10 times, twice a day.


3) For Back (Including CORE muscles)

- Superman exercise –
- Lying down prone on a mat àRaise both your arms and legs at the same time so that they are 10-12cm off the floor, forming a bowl shape with your body. Hold this position for 5 to 10 seconds then lower back to the starting position àRepeat for 10 times, Twice a day.
- Or lift contra lateral arm and leg at once, continue same as above.

- Plank Position
- maintain below position(similar to a push-up) – Back not curved, on your tiptoes and elbows for 10 seconds or maximum possible time à Twice a day.

Muscle Stretching Exercises
These exercises should be performed prior to Strengthening exercises as a part of a Warm Up setup. All active stretched positions (muscle fully lengthened position up to a firm end feel as felt by the person) should be held up to 10 to 15 seconds and to be slowly released. Repeat 2 to 5 times if necessary. Try to be in a seated or Lying down position as much as possible. Slowly perform the movement.
This is a very basic Illustration. Individual specific muscles or muscle groups stretching might be needed as per the patients condition.
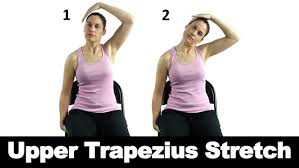
1) For Neck muscles
*Please avoid Hyper Extension of the neck if you are a diagnosed patient with Arthritis*

2) For Upper Limbs


3)For Trunk



4) For Lower Limbs







